Diabetes is one of the three leading causes of death worldwide and in Vietnam in recent years. According to WHO statistics, in 2016 there were 4.22 million people worldwide with diabetes problems not only in developed countries but also in low- and middle-income countries. Diabetes causes the death of 43% of elderly people aged 70 and over. Vietnam is currently one of the countries with a high prevalence of diabetes. It is estimated that by 2045, the proportion of people with diabetes will increase by 78% compared to the 2017 statistics to 6.3 million people, and the cost for the treatment of diabetes can amount to 1085.3 million USD/2045 (International Diabete Federation, 2018). Diabetes is currently classified into 3 groups: type 1 diabetes (the body is not able to produce insulin), type 2 diabetes (the body does not make enough and/or does not respond well to the insulin produced by the body) and gestational diabetes (a rise in blood sugar in the third trimester). Diabetes in general is very much related to the action of the hormone insulin, a hormone involved in the metabolism of carbohydrate compounds in the body, especially glucose from the blood to the cells. Diabetes can lead to dangerous complications in the eyes, heart, kidneys, nervous system and extremities. People with type 1 diabetes often require lifelong insulin therapy, while type 2 and gestational diabetes can be treated with medication, as well as a healthy diet and lifestyle.
In 1981 this concept was challenged with the introduction of the Glycemic Index (GI) which demonstrated that, despite equicarbohydrate amounts, foods may results in very different postprandial blood glucose repsonses. The GI allow the ranking of carbohydrate containing foods based on the glycemic response they illicit when consumed. The GI of a given food is determined by the blood glucose tolerant test, blood glucose is measured at regular intervals over a two – hour period following consumption. The glycemic index is caculated as the area under the glucose curve of the test food, divided by the pressed as a percent. The generally accepted convention is that foods with a GI of 55 or less are considered to be “low GI”, foods with a GI between 56 and 69 are consiederd “medium GI” , and foods with a GI above 70 are considered as “high GI”.
    |
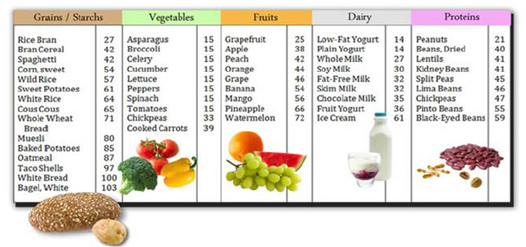 |
| The glycemic index of some foods |
Mechanisms of High GI and Low GI diets
The metabolic effeccts of low and high GI diets are hypothesis to be related to the rate of glucose absorption from the small intestine. The rapid rate of glucose absorption aftere consumption of a high- GI meal causes a spike in blood glucose concentration. This transient hyperglyceia stimulates the rapid release release of insulin from pancreatic beta cells and simultaneously inhibit secretion of glucagon from pancreatic alpha cells. The rise inninsulin secretion facilitates the uptake of glucose by the liver, muscle, adipose and other insulin-dependent tissues, thus quickly lowering blood glucose levels. However, two to four hours after a high-GI meal the high insulin and low glucagon levels result in blood glucose levels falling below starting levels often into the hypoglycemic range. In turn, this stimulates a counter regulatory hormone response to achieve normal glycemic levels and increases glycogenolysis and gluconeogenesis. As a result, high-GI carbohydrates increase the concentration of free fatty acids, which causes insulin resistance and impaired glucose tolerance in subsequent meals. Furthemore, the hypoglycemia following the consumption of high-GI foods may induce feelings of hunger and may even preferentially stimulate the consumption of more high-GI foods, thus perpetuating the vicious cycle. In contrast, hypoglycemia does not occur during the postprandial period after consumption of low-GI carbohydrates due to a slower and more gradual absorption of glucose from the gastrointestinal tract. Consequently, there is less stimulus for insulin release, lower levels of free fatty acid and an increase in insulin sensitivity. The effects of ingesting a low GI meal may therefore impact the metabolic response to the next meal. The mechanisms for this “second-meal effect” are likely mediated by slower rates of absorption and digestion, which result in a delayed period of fasting between meals. The ingestion of a low-GI food at bedtime has been shown to suppress both nocturnal free fatty acid levels and postprandial glucose levels at breakfast, possibly due to reduced nocturnal lipolysis. A low-GI food taken in the evening can also prevent nocturnal hypoglycemia in patients with insulin-dependent diabetes mellitus.
|
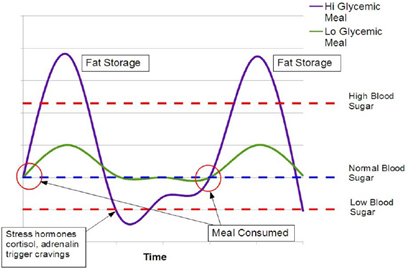 |
| Blood glucose levels when tolerating food |
More recently, reduced oxidative stress has been proposed as an additional mechanism by which low-GI foods attenuate insulin sensitivity and blood glucose levels. Oxidative stress is defined as a disturbance in the balance between the production of free oxygen radicals and antioxidant capacity. For a healthy diet, especially people with diabetes, obesity and insulin resistance, it is recommended to choose foods with a low glycemic index; Because these foods will help blood glucose not increase after eating, regulate lipoproteins in the blood (Brand Miller, 2002; Heibram, 2002). These effects will be shown to be effective in reducing diabetes-related metabolic diseases such as cardiovascular disease, high blood pressure, bone and joint diseases.
References:
1. Brand-Miller, J. C., Holt, S. H., Pawlak, D. B., & McMillan, J. (2002). Glycemic index and obesity. The American journal of clinical nutrition, 76(1), 281S-285S.
2. Heilbram LK va CS (2002). The effect of high and low - glycemic index energy restricted diets on plasma lipid and glucose profiles in type 2 diabetic subjects with varying glycaemic control. J Am coll Nutr 21, 120-127.
3. International Diabetes Federation, 2018
4. Rahelić, D., Jenkins, A., Božikov, V., Pavić, E., Jurić, K., Fairgrieve, C., ... & Vuksan, V. (2011). Glycemic index in diabetes. Collegium antropologicum, 35(4), 1363-1368.
5. WHO, 2016. Global report for Diabete. https://www.who.int/publications/i/item/9789241565257
Msc. Nguyen Thi Quyen- Department of Food Processing Technoloogy